


At Pelvic Therapy Specialists we work with a variety of patients who experience low back, hip, and pelvic dysfunction. A large subgroup of our patients includes post-partum women who are eager to get back into exercise. Living in such an active area creates additional pressure to get back in shape sooner than when your body might be ready. This article includes 6 popular myths about returning to running post-partum and 5 exercises to get you started in your post-partum rehab… yes rehab, you’re body just went through a lot, 10 months of physical changes to be exact, so it is important to give your body adequate time to heal and ensure that you are returning to exercise safely.
Myth #1:
It’s okay to start running after you’ve had your 6-week post-partum checkup.
Myth #2:
It’s normal to experience urinary incontinence while running after you’ve had a baby.
Myth #3:
If I can do a kegel, then I’m strong enough to run.
Myth #4:
It is safe to return to running if I have a prolapse and my pelvic floor is strong.
Myth #5:
I should not be running if I have an abdominal separation.
Myth #6:
Running downhill takes less effort and is therefore easier on my body.
Now that we have some myths out of the way, let’s dive a bit more into the research. This myth demystifying includes both evidence-based research and some of my clinical experience.
MYTH #1: IT’S OKAY TO START RUNNING AFTER YOU’VE HAD YOUR 6-WEEK POST-PARTUM CHECKUP.
FACT #1
Your 6-week checkup is really the green light to start your rehab… not to start running. Prior to your 6-week checkup, you are focused on healing and of course taking care of your baby. Patients can return to running at 3-6 months post-partum at the earliest. If you’ve had a vaginal delivery, research suggests that recovery of the pelvic floor muscles and associated connective tissues is usually achieved by 4-6 months post-partum. If you had a cesarean section, you may need more time. The abdominal fascia has only regained 51%-59% of its original tensile strength by 6 weeks and 75% to 93% at 6-7 months.
Furthermore, you also need to consider that if you are breast feeding healing may also change. There will be an altered hormonal environment including lower levels of estrogen and higher levels of relaxin that lasts up to 3 months post weaning from breast feeding. Relaxin is a hormone that loosens the ligaments in the pelvis to prepare your body for childbirth. Having this present in your body post-partum may make you more prone to tissue injury. Thus, it is important to give your body adequate time to heal. Running is not recommended for at least 12 weeks post-partum.
MYTH #2: IT’S NORMAL TO EXPERIENCE URINARY INCONTINENCE WHILE RUNNING AFTER YOU’VE HAD A BABY.
FACT #2
I always say to my patients that urinary incontinence may be common, but that does not mean that it is normal. Urinary incontinence is leakage of urine. A common type of urinary incontinence that occurs in post-partum women is stress urinary incontinence (SUI) which typically occurs with activities like coughing, sneezing, laughing, jumping, etc. The cause of SUI can be multi-factorial. It can be due to excessive intra-abdominal pressure, weakness in the pelvic floor muscles, laxity in the tissues supporting the pelvic organs, and/or a coordination/timing issue. If you are leaking urine with exercise it means that something in the system is not working correctly. This leaking may be benign in some but could be predisposing your body to further injury if not addressed early on. It is important that as you begin your journey to return to running that you don’t ignore these issues. Other complaints that may be a yellow flag include fecal incontinence or leakage of stool, fecal or urinary urgency, heaviness/pressure/dragging in the pelvic area, pain with intercourse, and musculoskeletal pain. In summary, leakage may be a sign that you are not yet ready to return to running as it is a sign that the pelvic floor and core muscles are not working optimally.
MYTH #3: IF I CAN DO A KEGEL, THEN I’M STRONG ENOUGH TO RUN.
FACT #3
Just being able to do a kegel or contract your pelvic floor muscles does not mean you are strong enough to run. As pelvic therapists we measure your pelvic floor strength and make sure you are not only strong enough to lift up your pelvic floor against gravity, but that you are also strong enough to tolerate impact. When you walk or run you exert force on the ground and the ground exerts and equal and opposite force onto you. This is called the ground reaction force. This force will increase with running compared to walking, running faster compared to slower, and running downhill compared to running on a flat surface. Running can cause a ground reaction force that can be up to 2-3x your body weight. Having adequate strength and endurance in your pelvic floor muscles is key to providing you with pelvic organ support and adequate core stability. It is also important that you have strength in your lower extremity muscles to support your pelvis and control where your limbs move as your absorb shock from landing on one leg at a time. Your rehab should include an adequate strength assessment of your core and lower extremity musculature to ensure a safe return to running.
MYTH #4: IT IS SAFE TO RETURN TO RUNNING IF I HAVE A PROLAPSE AND MY PELVIC FLOOR IS STRONG.
FACT #4
Just being able to do a kegel or contract your pelvic floor muscles does not mean you are strong enough to run. As pelvic therapists we measure your pelvic floor strength and make sure you are not only strong enough to lift up your pelvic floor against gravity, but that you are also strong enough to tolerate impact. When you walk or run you exert force on the ground and the ground exerts and equal and opposite force onto you. This is called the ground reaction force. This force will increase with running compared to walking, running faster compared to slower, and running downhill compared to running on a flat surface. Running can cause a ground reaction force that can be up to 2-3x your body weight. Having adequate strength and endurance in your pelvic floor muscles is key to providing you with pelvic organ support and adequate core stability. It is also important that you have strength in your lower extremity muscles to support your pelvis and control where your limbs move as your absorb shock from landing on one leg at a time. Your rehab should include an adequate strength assessment of your core and lower extremity musculature to ensure a safe return to running.
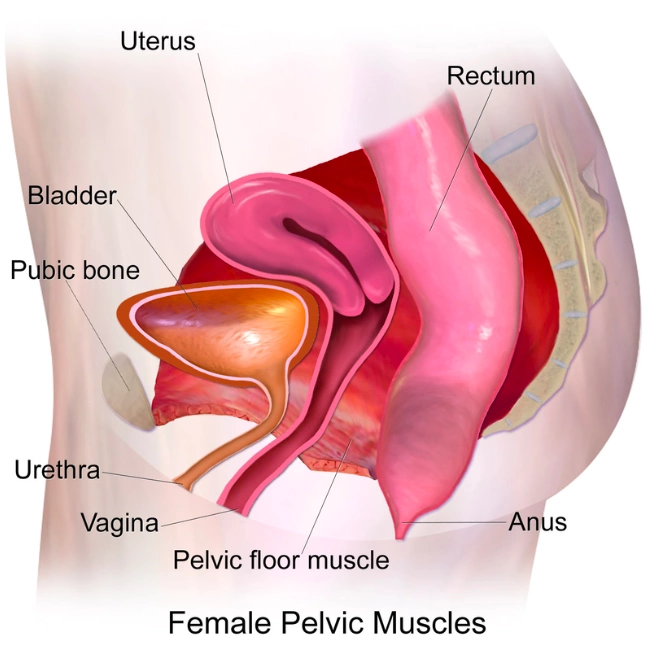
When it comes to pelvic organ support there are several key factors that come into play. Your pelvic organs include your bladder, uterus/vagina, and rectum which run from front to back (see photo). Support comes from ligaments and fascia which surround these organs and anchor them to your pelvis and neighboring structures. The pelvis is open at the bottom, which allows for childbirth, but does make for a compromised support system if the pelvic floor is not strong and or if the ligaments/fascia supporting the organs become stretched during pregnancy and delivery. During your post-partum physical therapy visit, we must consider your pelvic floor strength in addition to support from passive structures (i.e. ligaments/fascia) to determine if you may benefit from a pessary as you begin your rehab journey. A pessary is an orthotic that is inserted vaginally to provide additional support to the pelvic organs. This will typically be fitted by your OBGYN.
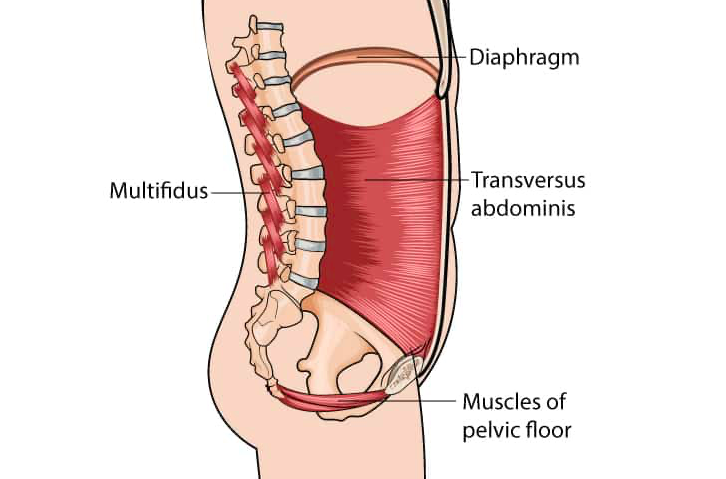
In addition to pelvic support, it is also important to look at support of the core as a whole. The core includes your diaphragm up top, transversus abdominus in the front, pelvic floor on the bottom, and multifidus in the back. I like to think of it as the roof, floor, and walls of your house. These muscles are key in stabilizing your trunk as well as managing intra-abdominal pressure. If there is a separation or weakness anywhere in your core it will impact the other muscles as well. Think of trying to squeeze a can of soda before opening it (strong core) and after opening it (weak core). More on this in the next myth buster.
MYTH #5: I SHOULD NOT BE RUNNING IF I HAVE AN ABDOMINAL SEPARATION.
FACT #5
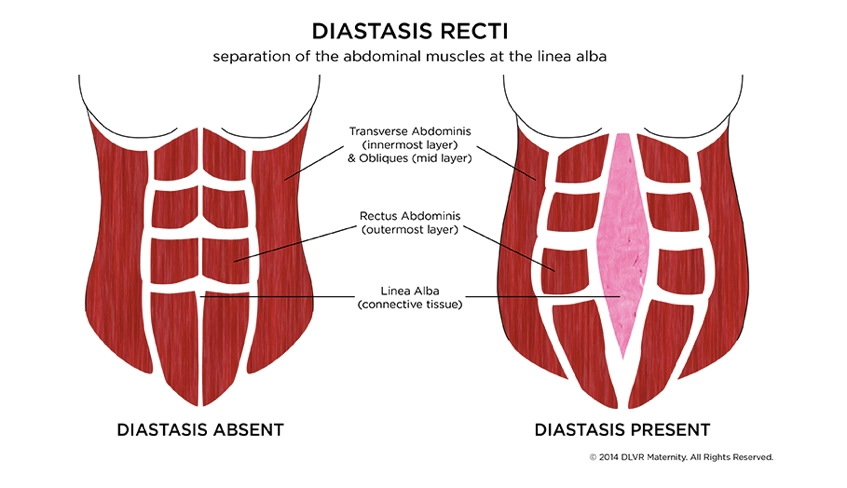
An abdominal separation or diastasis recti is a split in the abdominal wall between the two bellies of the rectus abdominus or “6 pack” muscles in your abdomen. Diastasis recti occurs in almost 100% of pregnant women. Yes, you read it right. As your baby grows your belly expands to accommodate the growth and it is normal to experience an abdominal separation during this time, especially during your third trimester. In many women the diastasis recti will heal on its own, but in some, core strengthening is necessary to regain tension through the abdominal wall. When rehabbing your abdominal separation, we are not only looking at the distance between the two muscles bellies, we are also looking at the tension generated through the linea alba, which is a fibrous structure that runs down the midline of the abdomen and serves as an attachment point for your abdominal muscles. You can be fully functional with a larger separation as long as you are able to generate adequate tension, think back to the empty can full can example in the previous section. When evaluating a diastasis recti we look at the finger width distance, finger width depth, and ability to tolerate loading by challenging the core in a variety of positions. Simply having a separation does not mean that your core is weak.
MYTH #6: RUNNING DOWNHILL TAKES LESS EFFORT AND IS THEREFORE EASIER ON MY BODY.
FACT #6
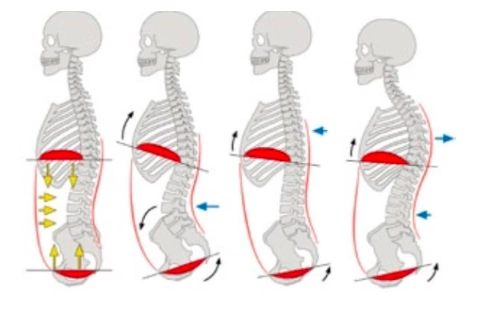
As previously mentioned in this article running downhill increases the ground reaction force which essentially means there is a larger impact on your body. In addition, running downhill can change the relationship of the diaphragm and the pelvic floor which can impact how you recruit your pelvic floor muscles. The pelvic floor and the core as a whole work optimally in a neutral spine position. As you are running downhill the tendency is to lean back to control your speed, which can negatively impact the ability to recruit your pelvic floor. Try standing up on your feet and play with shifting your weight forward into your toes and backwards into your heels. Then try performing a kegel in these different positions. Notice a difference in where you might feel the squeeze pressure. While returning to running, strength in the core and lower extremities is as important as paying attention to proper positioning. Having the diaphragm over the pelvic floor ensures proper support on impact.
